Travel Vaccines
Malaria Tablets
What is it?
Malaria is a common and life-threatening disease that affects thousands of travellers every year. It is spread through the bite of an infected mosquito, of which there are five different species worldwide that can spread the disease to humans. Mosquitos that transmit malaria, normally feed from sunset to sunrise. Symptoms of malaria may vary but include fever, headache, fatigue and muscle aches.
Risk areas
Malaria is widely distributed in tropical regions around the world, including parts of Africa, Asia, Central and South America, the Carribean and the Middle East.
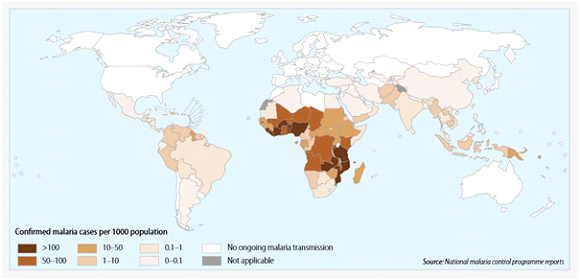
All travellers to countries or areas where malaria occurs are at risk of infection. Migrants to the UK that were born in malaria risk areas are at high risk when visiting friends and relatives in their country of birth. This is because of an assumption that they have immunity from having being born there. Immunity however, disappears very quickly upon moving to an area with no malaria risk.
Prevention
Prevention of malaria follows four important steps:
- Awareness of the risk (understanding if travelling to an area of risk)
- Bite prevention (particularly at nighttime)
- Chemoprophylaxis (use of appropriate malaria prevention tablets)
- Diagnosis (prompt recognition of symptoms and treatment)
Choice of malaria tablets
The choice of tablets is dependent upon the type of malaria present in the area visited and if there is any resistance to any of the available medicines.
We can provide medication to prevent malaria that is appropriate for the area of the world you are visiting. We also make sure you know what steps to take to help avoid insect bites, including the use of WHO recommended insect repellents.
Cholera
What is it?
Cholera is bacterial infection that is characterised by watery diarrhoea. It is commonly caused by contaminated food and water.
Risk areas
Common in many low-income countries and is associated with poor sanitation and poor access to clean water. The overall risk for travellers is very low but the risk is far greater for those living in unsanitary conditions, for example relief workers in disaster or refugee areas.

The disease is endemic in Africa, Asia, Central and South America and is prevalent in areas where there is poor sanitation.
Prevention
Following good personal hygiene and safe food and water practices can help reduce the risk of acquiring cholera.
Vaccine schedule
Dukoral, a licensed vaccine effective against cholera, is available in the UK. It is not recommended for most travellers but for those whose activities or medical history puts them at increased risk. This includes:
- Aid workers
- Those going to areas of cholera outbreak and who will have limited access to safe water
| Age | Primary course |
|---|---|
| Adults &children older than 6 years | 2doses at least one week apart. If more than six weeks have passed between doses, the primary course should be restarted. |
| Age 2 to 6 years | 3doses at least one week apart. If more than six weeks have passed between doses, the primary |
| course should be restarted. |
DTP
What is it?
The combined injection protects against three different diseases. Tetanus is a vaccine-preventable disease that is caused by toxins produced by bacteria found in soil worldwide. Polio is a potentially paralyzing, vaccine preventable viral infection that is transmitted through food or water contaminated by human faeces or direct contact with an infected person. Diptheria is a bacterial infection that is spread by exhaled water droplets, especially when in close contact with local population of endemic countries.
Risk areas
Tetanus is found worldwide but is generally more common in countries with poor vaccination coverage. Polio is now only endemic in Afghanistan and Pakistan but it can be imported to other countries by infected individuals. Diptheria can be found worldwide but is more common in developing countries where vaccination coverage is not as widespread.
Vaccine schedule
Travellers should have completed or be up-to-date with a primary vaccination course according to the NHS vaccination schedule.
| Vaccine | Schedule |
|---|---|
| Diptheria/Tetanus/Polio (Revaxis) | Single dose booster (if completed primary vaccination course)* |
*The primary course of diphtheria, tetanus and polio (DTP) is part of the standard UK childhood immunisation programme. If you have received the primary course, you may need a booster of one dose. If you have not received a primary course previously, you may require a course of three vaccinations.
Length of protection
10 years
Hepatitis A & B (+ paediatric)
What is it?
Hepatitis A is a highly infectious virus that can cause inflammation of the liver. The virus is most commonly transmitted through food or water that has been contaminated by human faeces or by direct contact with an infected person.
Risk areas
Hepatits A occurs worldwide, but areas with high levels of infection include low-income countries where there is poor sanitation or hygeiene practices. High risk areas include:
- The Indian subcontinent
- Subsaharan and North Africa
- Parts of South East Asia
- South & Central America
- The Middle East
Prevention
The most common route of infection in travellers is consumption of contaminated food or water. Simple measures to reduce the risk of infection include
- drinking water from a sealed source or boiled water,
- avoiding ice made from unpurified water,
- avoiding salad that may be washed with tap water and
- ensuring food has been freshly cooked and is hot
Vaccine schedule
There are several effective Hepatitis A vaccines available for travellers who intend to visit areas where Hepatitis A is common. Some of these vaccines have been combined with Typhoid and Hepatitis B.
| Vaccine | Schedule |
|---|---|
| Hepatitis A | 2 doses, given 6 – 12 months apart |
| Hepatitis A + Typhoid | Hepatitis A + Typhoid 1 dose followed by a single hepatitis A vaccine 6-12 months later Adults 15 years and over |
| Hepatitis A + B | 3 doses, 0, 1, and 6 months 4 doses, days 0, 7 and 21, 4th dose at 12 months |
Length of protection
The duration of protection from a completed course of Hepatitis A vaccine is a minimum of 25 years.
Japanese Encephalitis
What is it?
Japanese Encephalitis is a mosquito borne illness that can cause inflammation of the brain, and is potentially fatal. It is spread through infected mosquitos mainly from sunset to sunrise.
Risk areas
Despite the name, Japanese Encephalitis is endemic in 24 countries across Asia and the Western Pacific, not just in Japan. It is most common in rural areas where there is rice growing and pig farming, although it can occur in urban areas too.

The risk to travellers is generally very low, however it can increase significantly for persons who intend to live or travel in risk areas for long periods of time or who visit rural areas during transmission seasons. It should be noted that even short trips (fieldwork, camping or night time exposure) can significantly increase the risk to travellers.
Prevention
Bite avoidance, especially between dusk and dawn, can help reduce the risk of getting Japanese Encephalitis.
Vaccine schedule
There is a licensed Japanese Encephalitis vaccine that is recommended forindividuals who plan to stay in rural areas where Japanese Encephalitis occurs during the main transmission season or those whose activities put them at greater risk.
| Age | Schedule |
|---|---|
| 2 months and over | 2 doses: day 0 and 28 |
| Adults aged 18 to 65 years | 2 doses: day 0 and 28
Accelerated schedule: day 0 and 7 (this is recommended only when time before exposure is very |
Meningitis
What is it?
Meningococcal disease is a uncommon but potentially life-threatening infection caused by different strains for a bacteria species (Men A, B, C, W, Y and X). Around 10% of the UK population carry the meningitis bacteria in their nose and throat. It is spread between individuals by kissing, sneezing, coughing or during close contact with a carrier. Carriers of the bacteria generally don’t have any symptoms but can develop the disease in certain cases.
Risk areas
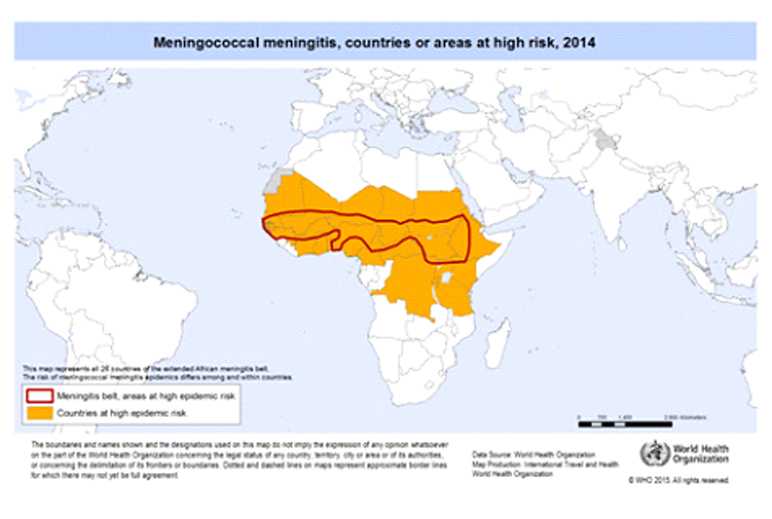
The disease is most common in the ‘meningitis belt’ of sub-Saharan Africa, stretching from Senegal through to Ethiopia. Following several large outbreaks of the disease in Saudi Arabia, certification of vaccination (with the quadrivalent vaccine) against Meningitis ACWY is now mandatory for pilgrims.
Prevention
Travellers to areas within the meningitis belt are at increased risk for a number of reasons such as:
- Long term stay with close contact with local population
- Healthcare workers
- Those visiting friends or relatives
- Backpackers
Vaccine schedule
| Age |
|---|
| Birth to less than one year |
| From one year of age (including adults) |
Length of protection
Booster dose can be considered after 5 years following primary vaccination.
Hajj & Umrah
We have plenty of experience vaccinating pilgrims travelling to perform Hajj and Umrah and our clinics are among those recommended by the Muslim Council of Britain (MCB). We can vaccinate you for Meningitis ACWY and give you the certificate required by Saudi Arabia for the visa. We can also offer other vaccines such as hepatitis A, hepatitis B and seasonal flu (at certain times of year) that are recommended by the Saudi Ministry of Health. Many of our staff have performed Hajj and are well placed to discuss questions you may have about your pilgrimage.
Rabies
What is it?
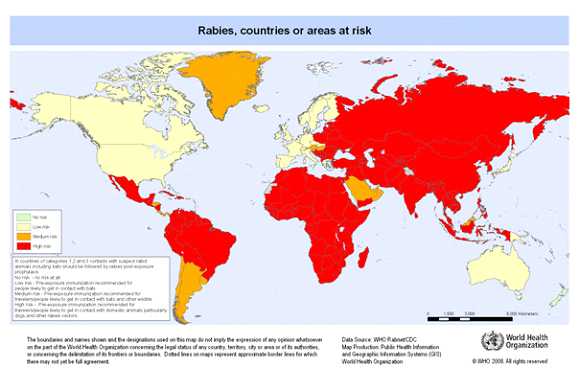
Rabies is a viral disease that is spread by a bite or scratch from an infected animal, usually a dog. It affects the brain and spinal cord and once symptoms are present, it is nearly always fatal. Rabies is estimated to caused around 60,000 human deaths worldwide each year.
Risk areas
Rabies is endemic throughout most of the world.
Prevention
Contact with wild or domestic animals should be avoided by travellers. The following steps should also be taken following potential rabies exposure:
- Immediately wash wound with soap & running water for several minutes
- Apply a disinfectant to the wound such as iodine or 40-70% alcohol
- Apply a simple dressing to the wound
- Seek medical advice as soon as possible
Vaccine schedule
Rabies vaccine is recommended for pre-exposure protection to travellers whose activities put them at increased risk. This includes:
- Those visiting areas where access to post-exposure treatment is limited
- Those planning high risk activities such as running or cycling
- Long-stay travellers (more than one month)
| Vaccine | Schedule |
|---|---|
| Rabies vaccine BP | 3 doses: Day 0, 7 and 28* *the 3rd dose can be given at day 21 if insufficient time before travel |
Length of protection
- Infrequent risk – booster dose to be considered at 10 years post primary course
- Frequent risk – booster at 1 year and then booster every 3 to 5 years
Tick Encephalitis (+ paediatric)
What is it?
Tick-borne encephalitis is a viral infection spread through the bite of an infected tick. It can also be spread via unpasteurized milk from infected cows, sheep and goats.
Risk areas
The disease occurs in parts of central, northern and Eastern Europe, Siberia and parts of Asia. In Europe, early spring through to late autumn are generally higher risk, however seasons vary by location. Travellers to areas where Tick-Borne Encephalitis is present may be at risk when walking, camping or working in woodland areas.
Prevention
Travellers should avoid known heavily tick-infested areas of forest and woodland during transmission seasons. Bite avoidance measures should also be employed when in risk areas and body should be checked regularly for ticks.
Vaccine schedule
Vaccination is available for all travellers to rural risk areas or those whose activities may put them at increased risk.
| Vaccine | Schedule |
|---|---|
| TicoVac & TicoVac Junior | 3 doses on days 0, between 1 and 3 months, and 5 to 12 months after the second dose (2nd dose can be given 2 weeks after 1st dose if necessary). |
Length of protection
First booster no more than 3 years after 3rd dose. After this, boosters may be given at 5 year intervals if at risk.
Typhoid
What is it?
Typhoid fever is a bacterial disease (Salmonella typhi or Salmonella paratyphi) that is spread by contaminated food and water. Symptoms include fever, headache, muscle or joint pains, constipation or diarrhoea and a rash. If treated, most people will make a full recovery however untreated it can be fatal.
Risk areas
Typhoid is found globally but mainly affects low income areas where sanitation is poor and clean drinking water is not widely available. The majority of cases occur in Asia (especially in travellers visiting friends and relatives in the Indian subcontinent) but is also a concern in parts of Africa, Central and South America.
Prevention
The risk can be reduced by ensuring good personal hygiene and practicing safe food and water advice.
Vaccine schedule
Vaccination is recommended for travellers who are at higher risk of infection in areas where sanitation and food hygiene are likely to be poor.
| Vaccine | Schedule |
|---|---|
| Typhoid (injection) | Single dose |
| Typhoid (oral) | 3 capsules; 1st on day 1, 2nd on day 3 and 3rd on day 5 |
| Hepatitis A &Typhoid | Single dose of combined vaccine |
Length of protection
Following a single dose of injection or completed course of oral vaccine, a booster should be offered at 3 year intervals depending on risk.
Yellow Fever
What is it?
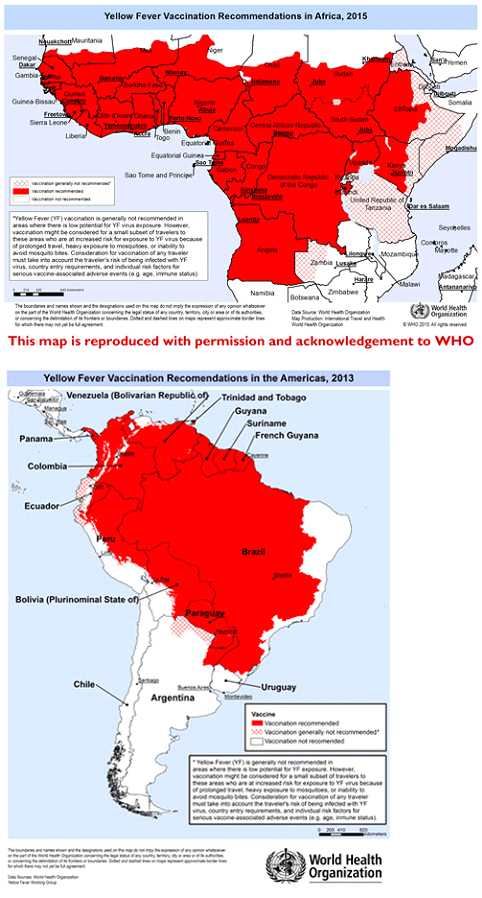
Yellow fever is a viral infection that is spread by certain species of day biting mosquitos. It can cause severe symptoms such as jaundice and damage to organs. During outbreaks, it can have mortality rates of up to 50% and so vaccination is recommended by the World Health Organization when travelling to risk areas.
Risk areas
YF is a risk in tropical parts of Africa, South America, eastern Panama in Central America and Trinidad in the Caribbean.
Prevention
Those visiting yellow fever risk areas should practice strict bite avoidance measures to help limit and reduce their risk.
Vaccine schedule
A highly effective live YF vaccine is available and in general vaccination is recommended for all persons visiting countries where there is a risk of YF virus transmission.We provide risk assessment, vaccination, advice and a yellow fever certificate if you receive the vaccine. If it is not appropriate for you to receive the yellow fever vaccine on medical grounds, we can provide an exemption certificate
| Vaccine | Schedule |
|---|---|
| Yellow Fever (Stamaril) | Single dose |
Length of protection
Protection against yellow fever following vaccination is life-long.
Chickenpox
What is chickenpox?
Chicken Pox is a highly contagious disease caused by the Varicella Zoster virus, and enters through your respiratory tract and conjunctiva.
How do you get chickenpox?
When exposed to an infected person, 9 out of 10 people will catch chickenpox. You can get it:
- When an infected person sneezes or coughs
- Through close contact with open blisters
People are most infectious 1-2 days before the rash appears and until all blisters have formed scabs.
Who is at risk from Chickenpox?
Chickenpox is a common childhood infection that is usually mild and complications rare. Almost all children develop lifelong immunity after infection, so most only get it once. The disease can have a more serious impact for certain people:
- Babies < 1 year
- Adults & adolescents > 15 years
- Pregnant women
- Individuals with a weakened immune system
What is the impact of Chickenpox?
There are estimated to be 670,000 cases of chickenpox every year, which is equivalent of one case every minute. It is generally a mild illness, but in some instances it can be associated with serious complications:
- Bacterial superinfections & severe scarring
- Pneumonia & bronchitis
- Ear infections
- Neurological disorders
Occasionally, chickenpox can be fatal, with the majority of deaths occurring in previously healthy individuals.
What is the chickenpox vaccine?
The chickenpox vaccine has been shown to provide immunity in 9 out of 10 children vaccinated. The vaccine is less effective after childhood, with an estimated three-quarters of adults & adolescents immune after vaccination.
Can I get the chickenpox vaccine via the NHS?
Unfortunately, the chickenpox vaccine is not part of the childhood immunization schedule, and is currently only given to people who are in close contact with someone that is particularly vulnerable to chickenpox.
Why not let my child get chickenpox naturally?
Chickenpox is a generally mild disease, but there is no way to know who will have a mild case or who will develop serious complications. The vaccine will provide immunity without the risk of serious complicationsof the disease. It will also prevent your child missing school, as chickenpox on average results in 6.6 days off school/childcare.
Combined MMR
What is it?
Measles, Mumps & Rubella are viral illnesses that are spread in the air by coughing or sneezing etc. They are highly infectious and can potentially cause serious and life threatening complications.
Risk areas
MMR are endemic in many countries around the world, and so pose a risk to all travellers. Countries in Asia and Africa often experience outbreaks, especially if there has been a natural disaster or conflict. The MMR vaccine is part of the UK childhood immunisation schedule, however many people may have missed their first or second dose and so are potentially at risk of disease.
Prevention
All unvaccinated individuals or those with incomplete vaccination should complete ensure the primary vaccination schedule is up to date
Vaccine schedule
| Age | Schedule |
|---|---|
| Adults &children over 6 months * | 2 doses: 0 and 1 month |
*This schedule is pertinent to those individuals that are unvaccinated or have an incomplete vaccination record. The NHS childhood schedule should be referred to for routine vaccination.
HPV
tbc
Influenza
tbc
Meningitis B
tbc
Shingles
tbc
Pneumococcal pneumonia
tbc
Nottingham
Nottinghamshire
NG7 3NS